Details on the objectives and methods as well as main results from the I.Family study as provided in the Final Project Report from April 2017 can be found here. In the following, these previous results were updated with more recent research findings from the IDEFICS/I.Family cohort. Lists of all publications from the IDEFICS study and the I.Family study are provided on the project websites (see above), under “Publications” and “Project publications”, respectively.
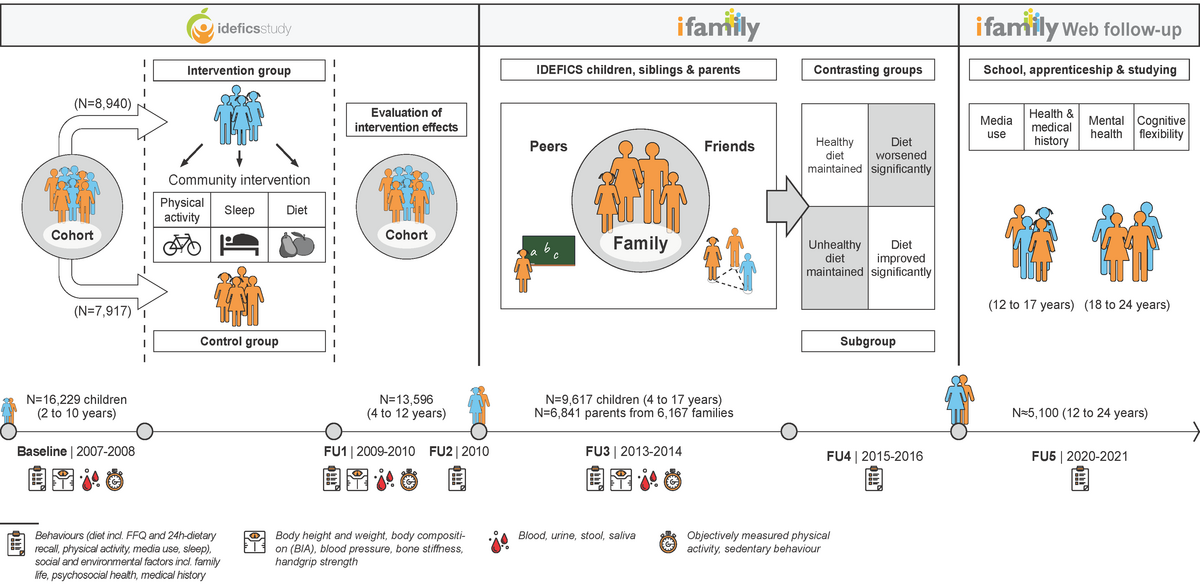
An overview of the survey waves of this large European cohort study with the number of participants, age ranges and the examinations and measurements carried out is given in Figure 1.
Impact of socio-economic status on prevalence/incidence of overweight/obesity
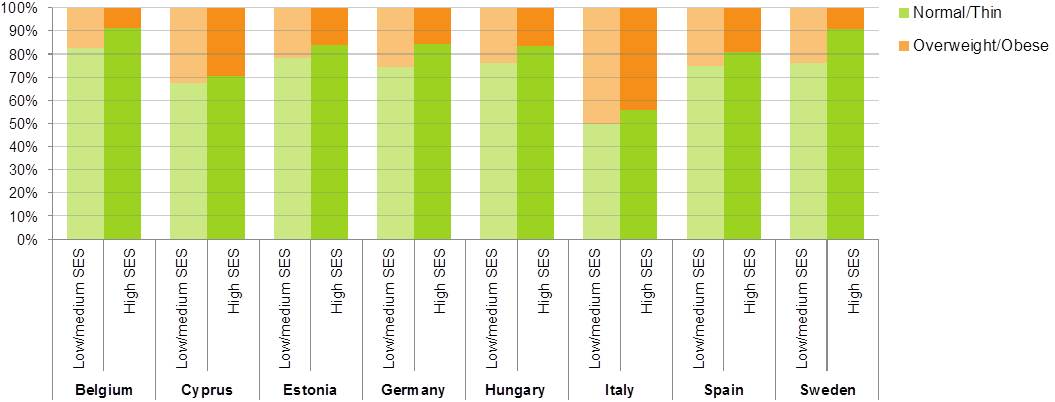
- In the study regions, the percentage of overweight/obese children differed between families of lower and higher socio-economic status (SES), but also between countries as shown in Figure 2 with a south-north gradient as also observed by other studies.
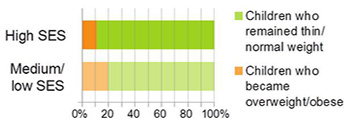
- As children grew up this effect got stronger. Figure 3 shows the incidence of overweight/obesity by socio-economic status (SES) over a six year period. In families of medium or low socio-economic status (SES), nearly twice as many as compared with high SES families.

Diet and children’s health
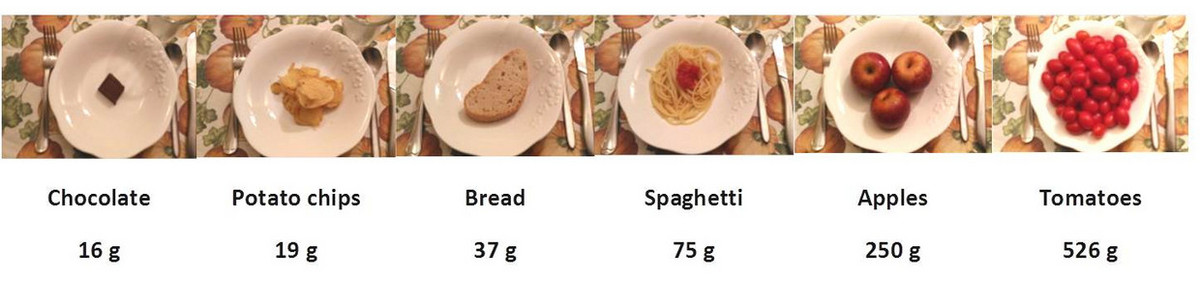
- On average, the children ate too much energy-dense food, where the consumption of such foods increased with age. The average energy density of foods eaten by I.Family children was about 2 kcal/g where an average energy density of about 1.25 kcal/g is considered as appropriate. Figures 4 and 5 show examples of popular foods among European children with relation to energy density and kilocalorie count.
- A healthy Mediterranean-type diet, rich in vegetables, legumes, fruits, nuts, cereals and fish and low in other animal products, was popular in 30-40% of children. It is noteworthy that this was particularly the case in Swedish children.1
- Sugar intake (all mono- and disaccharides) of children in I.Family was very high and made partly (e.g. in Germany) more than 30% of their total energy intake, irrespectively of being added or naturally occurring. The intake of total sugars as well as consumption of foods and drinks rich in added sugar were found to be higher on weekend days compared to weekdays.2
- Children with a diet high in vegetables, wholemeal cereals, fruit and plain milk, and low in sugary products had a lower incidence of overweight/obesity. After two years, the risk of becoming overweight/obese was reduced by 36% among children who adhered to this type of diet.3
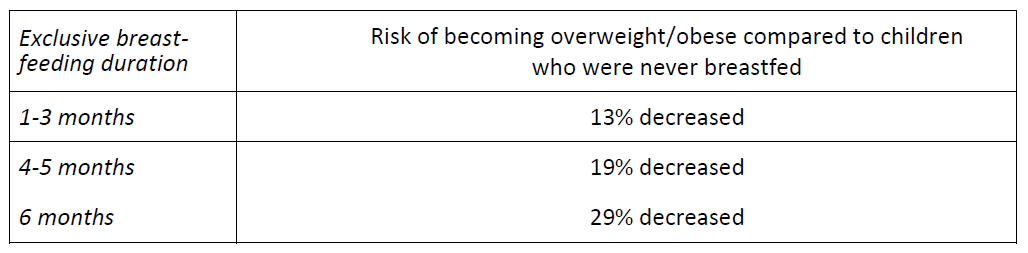
- Infant breastfeeding was associated with markers of metabolic health4 and reduced risk of childhood overweight5 (Table 1).
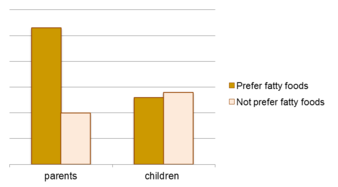
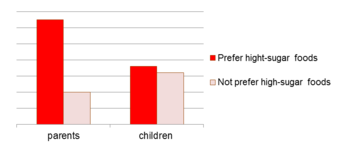
- Parents who preferred fatty foods consumed twice as many fatty foods compared to those who did not prefer fatty foods. This could be observed for sweet foods: parents who preferred sweet foods consumed three times as many sugar-rich foods compared to those who did not prefer sugar-rich foods. However, children’s food consumption seemed to be unaffected by their own preferences (see Figure 6).
- Across Europe, unfavourable parental consumer attitudes like trusting in advertisements or not avoiding additives were associated with a lower diet quality of their children.7
Media use
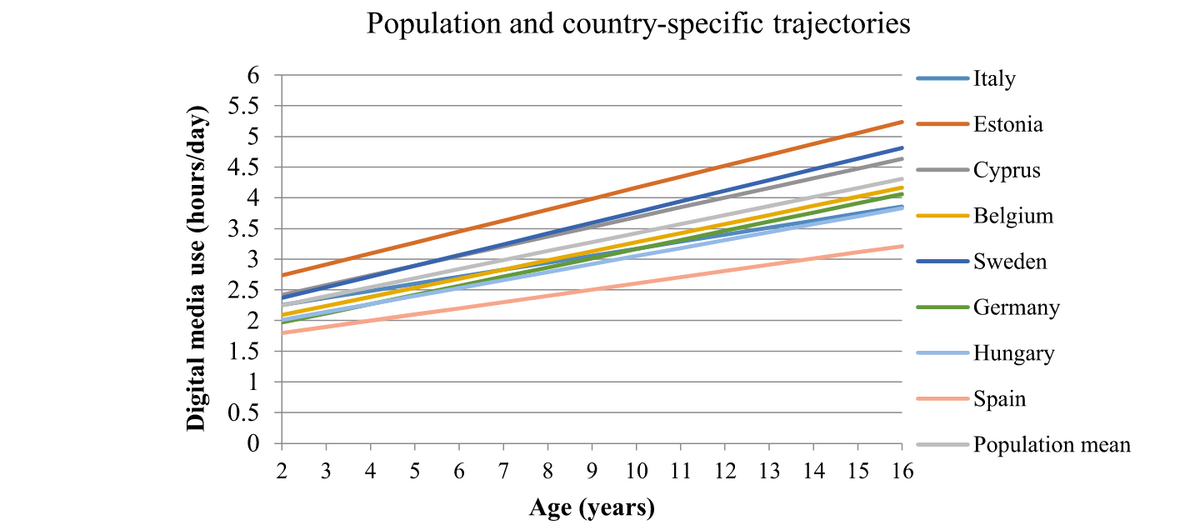
- Digital media use appears to be a risk factor for the development of metabolic disturbances in children and adolescents. Digital media exposure increased as children grew older (see Figure 7). Boys developed steeper digital media use trajectories and higher risk for metabolic disturbances compared to girls.
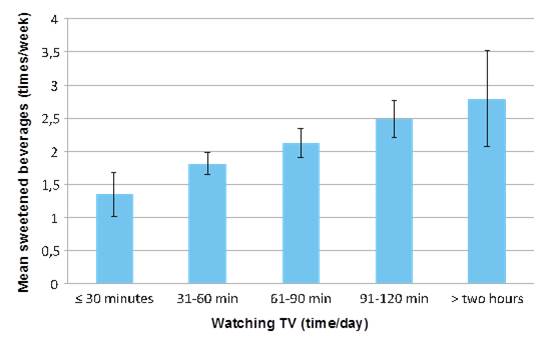
- A sub-study in Swedish children showed that TV advertising was a major factor encouraging children to eat unhealthy foods. Media influence was actually stronger than parental guidance in deciding what children eat. Children exposed to TV, especially commercial TV, consumed much more sweetened drinks (see Figure 8). This was observed regardless of whether parents discouraged such drinks or not.10
- Children who consumed meals while watching TV had a 20% greater risk of eating fatty foods and 30% greater risk of eating sugary foods compared to children who did not eat while watching TV. More surprisingly, we found that the effect of TV was the same for children who expressed high and low preferences for fats and sweets.11
Sleep patterns and associations with diet and health
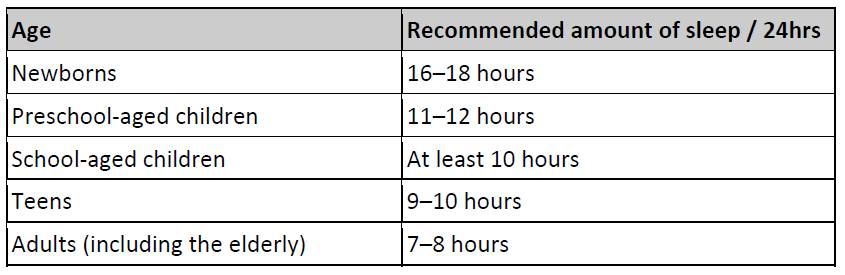
- Only one third of children and adolescents met the recommended sleep guidelines issued by the National Heart, Lung, and Blood Institute12 (Table 3). There was no difference between boys and girls.
- Children who met night-time sleep recommendations ate more vegetables than those not meeting the night-time sleep recommendations. Children who met the night-time sleep guidelines were also more likely to have healthy diets overall, as compared with those who did not meet the guidelines.
- A longer sleep duration was indirectly associated with lower insulin resistance through its beneficial effects on abdominal obesity. Therefore, a longer sleep duration may exert short and long term beneficial effects on glucose metabolism.13
- Inadequate sleep duration and poor sleep quality were associated with long-term detrimental effects on bone health in children and adolescents.14
Sleep and well-being – what are the relationships?
- Children with poor psychosocial well-being (in particular, emotional and behavioural problems, problems with friends or peers) were at greater risk of becoming overweight.15
- Overweight children were at greater risk of developing poor psychosocial well-being – in particular, worse emotional well-being, lower self-esteem, and problems in relationships with both family and friends.16
- A large body of evidence suggests that short sleep duration and poor sleep quality are risk factors for childhood overweight16. Our data support the observation that children with short sleep duration were at increased risk of being overweight.17
- Children whose well-being improved over time or stayed at a constant level tended to sleep longer at night as compared with children whose well-being worsened. In addition, they tended to have fewer difficulties in falling asleep and getting up in the morning.
- Furthermore, children who improved their night-time sleep duration or stayed at a constant level tended to have better well-being as compared with children whose sleep duration reduced. Children whose sleep quality remained good over time tended to have better well-being compared to those whose sleep quality worsened.
Children’s well-being matters
- Poor well-being increased themetabolic risk indirectly through diet, physical activity, sleep, and media use behaviors, as well as higher abdominal fat. Both cross-sectionally and longitudinally, higher levels of well-being showed indirect beneficial effects on blood pressure, glucose metabolism and blood lipids (triglyceride and high-density lipoprotein cholesterol).18
- A higher psychosocial well-being was associated with lower emotion-driven impulsiveness whereas a higher number of stressful life events was associated with higher emotion-driven impulsiveness. Therefore, well-being and stressful life events need to be further considered in the development and tailoring of health promotion strategies that aim to reduce emotion-driven impulsiveness.19 Reducing emotion-driven impulsivness can help to prevent obesity as adolescents with a stronger emotion-driven impulsiveness tendency reported a higher snacking frequency, specifically of more energy-dense snacks.20

Physical activity and children’s health
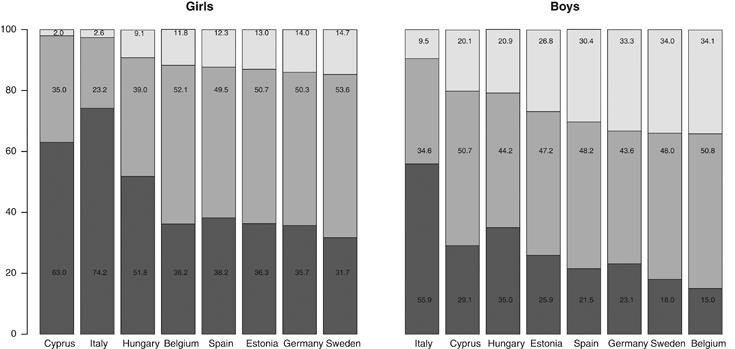
- Only a small proportion of young people in our 8 European study regions met current physical activity guidelines (Box 1) – to be at least moderately active for 60 minutes or more each day (Figure 9). The group with the highest percentage meeting the guidelines was Belgian boys – but still only 34% of them did so.
- Girls were less active than boys irrespective of how old they were. The daily duration of physical activity children declined at an average rate of 4.3% from the age of five to 15 years – a 4.1% per annum decrease in boys and a 4.5% per annum decrease in girls. Young people also became progressively more sedentary as they matured. At 5-7 years, they spent 40% of their time sitting, compared to 62% of their time at 14-16 years.
- The place of residence also affected the gender gap in physical activity. There was considerable variation in physical activity levels by country. The children in our Italian cohort were the least active, and the Sweden children the most active. The difference in average daily activity duration between the least active population (Italy) and the most active (Sweden) was larger than the difference we observed between boys and girls. Indeed, girls in the two most active countries (Belgium and Sweden) were more active than boys in the two least active countries (Italy and Cyprus).
- Children who met current physical activity guidelines [60 min moderate-to-vigorous physical activity (MVPA) daily] had a lower risk of becoming overweight over time compared to less active children. Similar associations were found for 45 min MVPA daily. On the other side, children who became overweight had the lowest odds to achieve 45 or 60 min MVPA daily compared to normal weight children. Thus, the associations between physical activity and weight status were bi-directional.23
- There was a weak trend towards increasing physical activity with increasing parental education and income in the full sample. This trend was similar across the eight countries. There were some differences in the social gradient for particular behaviours (e.g. active transport, organized sports). However, these did not necessarily show up when we looked at overall activity levels.
- Physical activity was clearly related in families in a straightforward way: more active children had more active parents and siblings. This relationship was strongest between siblings; it was not quite as strong when we compared parents/ carers and children.
- Physical activity seemed to be beneficial forbone health. In contrast, increasing durations of screen-based sedentary behaviors might be risk factors for poor bone health development, especially in children and adolescents with overweight/obesity.24
Local neighbourhoods – what difference do they make?
- For children, physical activity was encouraged by the availability of public open spaces within densely residential areas. However, this association was modified by safety concerns, age and sex. If parents felt that the neighbourhood was not safe for children, they tended to restrict children’s outdoor activity. This is especially true if their child is female.25
- For adolescents, good walking and cycling facilities as well as diverse destinations mattered, while public open spaces became less important. In addition, we know that physical activity declines sharply in the transition from childhood to adolescence. Our research showed that urban moveability counteracts this decrease in physical activity, but with some differences between boys and girls. Connectivity and availability of walking and cycling facilities as well as diverse destinations seemed to promote an active lifestyle in girls. For adolescent boys, public open spaces remained an important factor to support adequate physical activity.
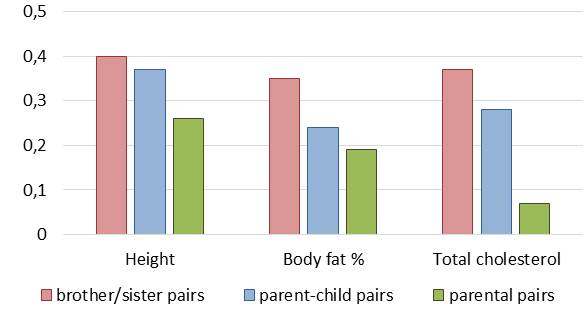
How family relations influence children’s health
- Family members resembled one another in terms of height, body fat measures and cardiovascular disease risk (e.g. total cholesterol) (Figure 10). Mothers tended to resemble their children more than fathers. The resemblance was stronger for biological relatives (sibling pairs, parent-child pairs) than non-biological relatives (parental pairs), which indicates that these traits are likely under strong genetic influence. Sibling correlations for body fatness and total cholesterol were stronger than parent-child correlations, which could be related with the environment shared by siblings.
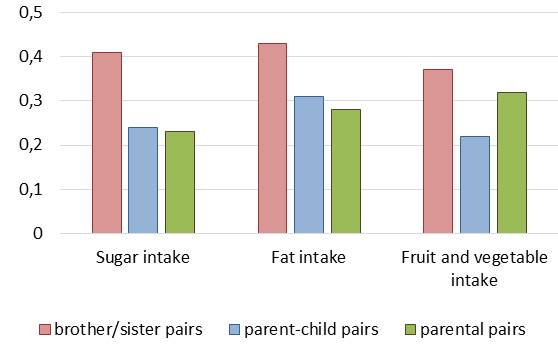
- Family members also had similar diets (Figure 11). Interestingly, the resemblance was strongest for sibling pairs and a bit less for parent-child and parental pairs. Since the correlation was similar in genetically related and non-genetically related family members, we may infer that the shared household is an important factor in dietary intake.
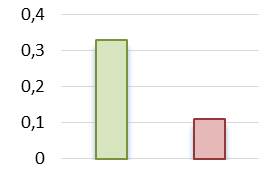
- Parents and their children had similar food intakes (Figure 12). This was especially true for the intake of healthy foods, but less so for the intake of unhealthy foods. One possible explanation might be that there are many external influences promoting unhealthy foods to children (e.g. supermarkets, advertising, pester power, etc.) in developed European societies but only few external influences for healthy foods.
- The home environment is likely to be the main factor explaining intake of healthy foods, including fruit and vegetables: If such foods were not available to children at home, children were unlikely to consume them outside the home with the possible exception of meals provided at school or daycare.
- Children had a higher natural preference for sweet tastes than adults. So it was not surprising that we saw more variation between children and parents when it came to eating unhealthy foods.
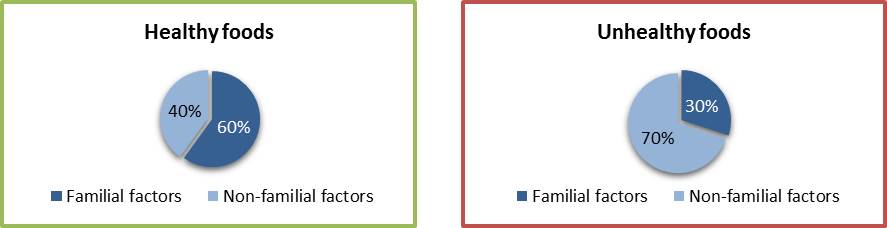
- Familial factors explained 60% of the variability in the intake of healthy foods but only half as much (30%) in the intake of unhealthy foods (see Figure 13).
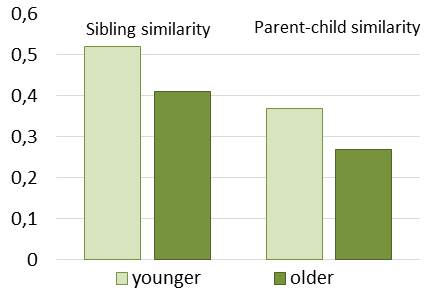
- In terms of the intake of healthy foods, there was a greater resemblance between younger sibling pairs (< 11 years) than older sibling pairs (≥ 11 years), and parents and their younger children (< 11 years) than parents and their older children (≥ 11 years) (Figure 14). It is likely that the frequency of family meals declines and that the influence of friends becomes more important as children become older and more independent.
How do friends affect teenagers’ health behaviours?
- Parents’ perception of their child’s weight was influenced by how much other children weighed. Parents perceived their child to be thinner than he or she was when their peers were heavier. The opposite effect occurred when other children around were slimmer.27
- Teenagers’ unhealthy food consumption was strongly associated with their friends’ unhealthy food consumption (sugar sweetened beverages, fatty foods, food high in sugar, fast foods). However, we did not observe an association for healthy foods among peers (vegetable/fruit consumption, fibre rich foods).28
- Patterns of sedentary behaviour and leisure time activity also tended to be similar between teenagers and their friends.28
Biomarkers and factors influencing metabolic health
- A high proportion of European children were vitamin D deficient. Time spent outdoors, UV radiation exposure and dietary vitamin D intake were important factors that may improve the vitamin D status.29
- Blood leptin concentrations were positively associated with insulin resistance and may prove to be useful in early detection of prediabetes.30
- Children who showed several metabolic syndrome components already as a young child have almost no chance to reach a healthy status later during childhood or adolescence. In this context we studied the role of lifestyle and nonmodifiable risk factors in the development of metabolic disturbances from childhood to adolescence: Especially less media devices in the bedroom, membership in a sports club, and a higher well-being seem to positively influence metabolic health.31,32
Role of genetic and epigenetic factors
- The results of a pilot study on a sub-sample of the I.Family cohort showed that a set of circulating microRNAs were differentially regulated in overweight/obese as compared with normal weight children.33
- Genetic predisposition to metabolic syndrome was observed to be largely driven by genes of obesity (FTO) and lipid metabolism (CETP). Therefore, inclusion of the associated genetic variants in polygenic scores for the metabolic syndrome may prove to be fundamental for identifying children and subsequently adults of the high-risk group to allow earlier targeted interventions.34
REFERENCES
- Tognon G, Hebestreit A, Lanfer A, Moreno LA, Pala V, Siani A, Tornaritis M, De Henauw S, Veidebaum T, Molnar D, Ahrens W, Lissner L. Mediterranean diet, overweight and body composition in children from eight European countries: cross-sectional and prospective results from the IDEFICS study. Nutr Metab Cardiovasc Dis. 2014;24(2):205-213.
- Svensson A, Larsson C, Eiben G, Lanfer A, Pala V, Hebestreit A, Huybrechts I, Fernandez-Alvira JM, Russo P, Koni AC, De Henauw S, Veidebaum T, Molnar D, Lissner L, consortium I. European children's sugar intake on weekdays versus weekends: the IDEFICS study. Eur J Clin Nutr. 2014;68(7):822-828.
- Pala V, Lissner L, Hebestreit A, Lanfer A, Sieri S, Siani A, Huybrechts I, Kambek L, Molnar D, Tornaritis M, Moreno L, Ahrens W, Krogh V. Dietary patterns and longitudinal change in body mass in European children: a follow-up study on the IDEFICS multicenter cohort. Eur J Clin Nutr. 2013;67(10):1042-1049.
- Priego T, Sanchez J, Pico C, Ahrens W, Bammann K, De Henauw S, Fraterman A, Iacoviello L, Lissner L, Molnar D, Moreno LA, Siani A, Tornaritis M, Veidebaum T, Palou A, Consortium I. Influence of breastfeeding on blood-cell transcript-based biomarkers of health in children. 10.1111/j.2047-6310.2013.00204.x doi. Pediatr Obes. 2014;9(6):463-470.
- Hunsberger M, Lanfer A, Reeske A, Veidebaum T, Russo P, Hadjigeorgiou C, Moreno LA, Molnar D, de HS, Lissner L, Eiben G. Infant feeding practices and prevalence of obesity in eight European countries - the IDEFICS study. S1368980012003850 pii ;10.1017/S1368980012003850 doi. Public Health Nutr. 2012:1-9.
- Fernandez-Alvira JM, Bornhorst C, Bammann K, Gwozdz W, Krogh V, Hebestreit A, Barba G, Reisch L, Eiben G, Iglesia I, Veidebaum T, Kourides YA, Kovacs E, Huybrechts I, Pigeot I, Moreno LA. Prospective associations between socio-economic status and dietary patterns in European children: the Identification and Prevention of Dietary- and Lifestyle-induced Health Effects in Children and Infants (IDEFICS) Study. S0007114514003663 pii ;10.1017/S0007114514003663 doi. Br J Nutr. 2015;113(3):517-525.
- Jilani H, Pohlabeln H, Buchecker K, Gwozdz W, De Henauw S, Eiben G, Molnar D, Moreno Aznar LA, Pala V, Reisch L, Russo P, Veidebaum T, Ahrens W, Hebestreit A, Consortium) obotIF. Association between parental consumer attitudes with their children’s sensory taste preferences as well as their food choice. PLoS One. 2018;1(13(8):e0200413)
- Hebestreit A, Intemann T, Siani A, De Henauw S, Eiben G, Kourides YA, Kovacs E, Moreno LA, Veidebaum T, Krogh V, Pala V, Bogl LH, Hunsberger M, Boernhorst C, Pigeot I, Consortium IF. Dietary Patterns of European Children and Their Parents in Association with Family Food Environment: Results from the I.Family Study. Nutrients. 2017;9(2):17.
- Sina E, Buck C, Veidebaum T, Siani A, Reisch L, Pohlabeln H, Pala V, Moreno LA, Molnar D, Lissner L, Kourides Y, De Henauw S, Eiben G, Ahrens W, Hebestreit A. Media use trajectories and risk of metabolic syndrome in European children and adolescents: the IDEFICS/I.Family cohort. Int J Behav Nutr Phys Act. 2021;18(1):134.
- Olafsdottir S, Eiben G, Prell H, Hense S, Lissner L, Marild S, Reisch L, Berg C. Young children's screen habits are associated with consumption of sweetened beverages independently of parental norms. 10.1007/s00038-013-0473-2 doi. Int J Public Health. 2014;59(1):67-75.
- Lissner L, Lanfer A, Gwozdz W, Olafsdottir S, Eiben G, Moreno LA, Santaliestra-Pasias AM, Kovacs E, Barba G, Loit HM, Kourides Y, Pala V, Pohlabeln H, de HS, Buchecker K, Ahrens W, Reisch L. Television habits in relation to overweight, diet and taste preferences in European children: the IDEFICS study. 10.1007/s10654-012-9718-2 doi. Eur J Epidemiol 2012;27(9):705-715.
- National Heart L, and Blood Institute. How much sleep is enough? Updated 24.03.2022. Accessed 20.07.2022, https://www.nhlbi.nih.gov/health/sleep/how-much-sleep
- Thumann BF, Michels N, Felso R, Hunsberger M, Kaprio J, Moreno LA, Siani A, Tornaritis M, Veidebaum T, De Henauw S, Ahrens W, Bornhorst C, Idefics, Consortia IF. Associations between sleep duration and insulin resistance in European children and adolescents considering the mediating role of abdominal obesity. PLoS One. 2020;15(6):e0235049.
- Cheng L, Pohlabeln H, Ahrens W, Russo P, Veidebaum T, Hadjigeorgiou C, Molnar D, Hunsberger M, De Henauw S, Moreno LA, Hebestreit A, Idefics, consortia IF. Cross-sectional and longitudinal associations between sleep duration, sleep quality, and bone stiffness in European children and adolescents. Osteoporos Int. 2021;32(5):853-863.
- Hunsberger M, Lehtinen-Jacks S, Mehlig K, Gwozdz W, Russo P, Michels N, Bammann K, Pigeot I, Fernandez-Alvira JM, Thumann BF, Molnar D, Veidebaum T, Hadjigeorgiou C, Lissner L, Consortium I. Bidirectional associations between psychosocial well-being and body mass index in European children: longitudinal findings from the IDEFICS study. BMC Public Health. 2016;16:949.
- Chen X, Beydoun MA, Wang Y. Is sleep duration associated with childhood obesity? A systematic review and meta-analysis. Obesity (Silver Spring). 2008;16(2):265-274.
- Hense S, Pohlabeln H, de HS, Eiben G, Molnar D, Moreno LA, Barba G, Hadjigeorgiou C, Veidebaum T, Ahrens W. Sleep duration and overweight in European children: is the association modified by geographic region? Sleep. 2011;34(7):885-890.
- Thumann BF, Börnhorst C, Ahrens W, Arvidsson L, Gwozdz W, Iguacel I, Mårild S, Molnár D, Rach S, Russo P, Tornaritis M, Veidebaum T, De Henauw S, Michels N. Cross-Sectional and Longitudinal Associations Between Psychosocial Well-Being and Cardiometabolic Markers in European Children and Adolescents. Psychosom Med. 2020;82(8):764-773.
- Do S, Coumans JMJ, Bornhorst C, Pohlabeln H, Reisch LA, Danner UN, Russo P, Veidebaum T, Tornaritis M, Molnar D, Hunsberger M, De Henauw S, Moreno LA, Ahrens W, Hebestreit A. Associations Between Psychosocial Well-Being, Stressful Life Events and Emotion-Driven Impulsiveness in European Adolescents. J Youth Adolesc. 2021;
- Coumans JMJ, Danner UN, Ahrens W, Hebestreit A, Intemann T, Kourides YA, Lissner L, Michels N, Moreno LA, Russo P, Stomfai S, Veidebaum T, Adan RAH. The association of emotion-driven impulsiveness, cognitive inflexibility and decision-making with weight status in European adolescents. Int J Obes (Lond). 2018;42(4):655-661.
- World Health Organization. Physical Activity. https://www.who.int/news-room/fact-sheets/detail/physical-activity
- Konstabel K, Veidebaum T, Verbesterl V, Moreno LA, Bammann K, Tornaritis M, Eiben G, Molnár D, Siani A, Sprengeler O, Wirsik N, Ahrens W, Pitsiladis Y. Objectively measured physical activity in European children: the IDEFICS study Int J Obes. 2014;38(Suppl 2):S 135-S 143.
- Sprengeler O, Pohlabeln H, Bammann K, Buck C, Lauria F, Verbestel V, Eiben G, Konstabel K, Molnar D, Moreno LA, Pitsiladis Y, Page A, Reisch L, Tornaritis M, Ahrens W. Trajectories of objectively measured physical activity and childhood overweight: longitudinal analysis of the IDEFICS/I.Family cohort. Int J Behav Nutr Phys Act. 2021;18(1):103.
- Cheng L, Pohlabeln H, Ahrens W, Lauria F, Veidebaum T, Chadjigeorgiou C, Molnár D, Eiben G, Michels N, Moreno LA, Page AS, Pitsiladis Y, Hebestreit A. Cross-sectional and longitudinal associations between physical activity, sedentary behaviour and bone stiffness index across weight status in European children and adolescents. Int J Behav Nutr Phys Act. 2020;17(1):54.
- Buck C, Tkaczick T, Pitsiladis Y, De Bourdehaudhuij I, Reisch L, Ahrens W, Pigeot I. Objective measures of the built environment and physical activity in children: from walkability to moveability. J Urban Health. 2015;92(1):24-38.
- Bogl LH, Mehlig K, Intemann T, Masip G, Keski-Rahkonen A, Russo P, Michels N, Reisch L, Pala V, Johnson L, Molnar D, Tornaritis M, Veidebaum T, Moreno LA, Ahrens W, Lissner L, Kaprio J, Hebestreit A. A within-sibling pair analysis of lifestyle behaviours and BMI zscore in the multi-centre I.Family study. Nutr Metab Cardiovasc Dis. 2019;
- Gwozdz W, Sousa-Poza A, Reisch LA, Bammann K, Eiben G, Kourides Y, Kovacs E, Lauria F, Konstabel K, Santaliestra-Pasias AM, Vyncke K, Pigeot I. Peer effects on obesity in a sample of European children. Econ Hum Biol. 2015;18:139-152.
- Gwozdz W, Nie P, Sousa-Poza A, DeHenauw S, Felső R, Hebestreit A, Iguacel I, Lissner L, Lauria F, Page A, Reisch LA, Tornaritis M, Veidebaum T, Williams G, Foraita R, Consortium obotIF. Peer Effects on Weight Status, Dietary Behaviour and Physical Activity among Adolescents in Europe: Findings from the I.Family Study. Kyklos. 2019;72(2):270-296.
- Wolters M, Intemann T, Russo P, Moreno LA, Molnar D, Veidebaum T, Tornaritis M, De Henauw S, Eiben G, Ahrens W, Floegel A. 25-Hydroxyvitamin D reference percentiles and the role of their determinants among European children and adolescents. Eur J Clin Nutr. 2021;
- Nagrani R, Foraita R, Wolters M, De Henauw S, Marild S, Molnar D, Moreno LA, Russo P, Tornaritis M, Veidebaum T, Ahrens W, Marron M, Idefics, consortia IF. Longitudinal association of inflammatory markers with markers of glycaemia and insulin resistance in European children. Diabetes Metab Res Rev. 2022;38(3):e3511.
- Börnhorst C. Metabolic status in children and its transitions during childhood and adolescence - The IDEFICS/I.Family study. Int J Epidemiol. 2019;
- Börnhorst C, Russo P, Veidebaum T, Tornaritis M, Molnar D, Lissner L, Marild S, De Henauw S, Moreno LA, Floegel A, Ahrens W, Wolters M. The role of lifestyle and non-modifiable risk factors in the development of metabolic disturbances from childhood to adolescence. Int J Obes (Lond). 2020;
- Iacomino G, Russo P, Stillitano I, Lauria F, Marena P, Ahrens W, De Luca P, Siani A. Circulating microRNAs are deregulated in overweight/obese children: preliminary results of the I.Family study. Genes Nutr. 2016;11:7.
- Nagrani R, Foraita R, Gianfagna F, Iacoviello L, Marild S, Michels N, Molnar D, Moreno L, Russo P, Veidebaum T, Ahrens W, Marron M. Common genetic variation in obesity, lipid transfer genes and risk of Metabolic Syndrome: Results from IDEFICS/I.Family study and meta-analysis. Sci Rep. 2020;10(1):7189.
Official project websites:
www.ideficsstudy.eu and www.ifamilystudy.eu
Contact:
i.family(at)leibniz-bips.de