
In order to be able to competently assess the health and nutritional status of a child regarding the existence of metabolic syndrome (MetS) based on a medical examination, it is necessary that different metabolic markers and anthropometric characteristics are measured. For the final evaluation of the examination results there are established thresholds and reference values for adults on which the doctor can orientate his/her diagnosis. However, such reference values are not available for children.
Three commonly used definitions for children were suggested by Cook et al. (1), Viner et al. (2) and the IDF (International Diabetes Federation) (3). Each of the definitions is based on the assessment of the following four components and major risk factors of metabolic syndrome: (1) excess adiposity, (2) blood pressure, (3) blood lipids (poor cholesterol values), and (4) elevated glucose/insulin. According to all three definitions a child is diagnosed with MetS if a predefined critical value is exceeded for three or all four of the stated risk factors. There are however some marked differences when it comes to the setting of the critical values (cut-offs), resulting in differences in the weighting of the risk factors as well as in the establishment of a diagnosis. The following figure illustrates this using the example of data from the IDEFICS study. When the three afore-mentioned definitions, with their respective thresholds for adiposity, blood pressure, lipids, respectively, glucose/insulin, are applied to the IDEFICS cohort, it can be seen e.g. especially according to the definitions by Cook et al. and Viner et al., that only a few children exceed the pre-determined threshold for glucose, respectively, insulin. As a result these components are accorded almost no relevance in the definition of metabolic syndrome. The same applies for the influence of elevated blood pressure values in the IDF definition: Due to the fact that the selected cut-offs are relatively high, only a few children will be classified as ”abnormal”, as a result blood pressure only has little influence in the IDF definition of metabolic syndrome. Furthermore, in all definitions it is most likely that the lipids threshold will be exceeded.

Based on data from the IDEFICS study (4), a multi-center, European study of children aged 2 – 10.9 years, a reference system supposed to fulfill the following requirement was derived in 2014 (5):
- During the diagnosis of metabolic syndrome each of the afore-mentioned major risk factors will be weighted equally (currently there is no clear indication as to whether one or more of these components has a stronger influence than the others).
- For the setting of the thresholds, only sex and age-specific cut-offs will be used (because the considered variables for the characterization of risk factors are strongly influenced by sex and age).
 body mass index cut‐offs for thinness, overweight and obesity. Pediatric Obesity. 2012;7(4):284-294.")
Measurement methods and exclusion criteria used in the IDEFICS study
To derive percentile curves for normal-weight children, restrictions regarding weight status had to be made for some markers that are associated with body weight. Table 1 shows the variables used in the online tool with the exclusion criteria used during the derivation of the percentile curves, as well as the measurement methods used.
Two definitions (Monitoring Level and Action Level) of metabolic syndrome based on percentiles derived from the IDEFICS study
Using a recently developed statistical approach, the GAMLSS-method (6), we derived sex- and age-specific percentiles for variables commonly considered to sufficiently characterize the four major cardiovascular risk factors and components of MetS in daily practice. Based on these percentiles we now suggest that the development of a child be closely monitored (‘Monitoring level’), respectively, that appropriate pediatric interventions are initiated (‘Action level’), when the values of at least three of the monitored risk factors exceed the 90th or the 95th percentile.
Table 1 shows the four components of metabolic syndrome as well as the suggested cut-offs for the characterization of ‘monitoring level’ and ‘action level’ for the variables waist circumference, blood pressure, triglycerides, high density lipoprotein (HDL) cholesterol, HOMA, and fasting glucose.
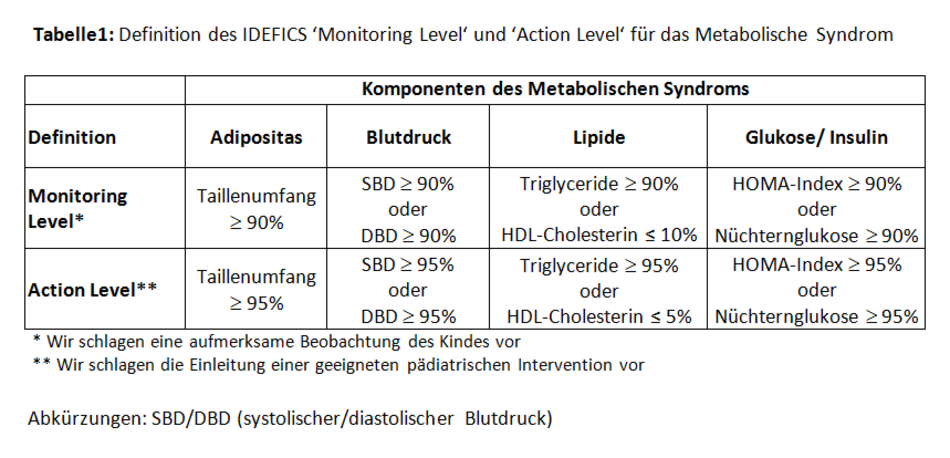
When these two definitions based on age- and sex-specific percentiles are applied to the IDEFICS study, it can be seen that the contribution of the 4 components is considerably more even than in the three definitions from Cook et al. (1), Viner et al. (2), or the International Diabetes Federation (IDF) (3), mentioned before. The fact that for the individual components, not exactly 10% (Monitoring Level), respectively 5% (Action Level) lie above the respective 90th, respectively 95th percentiles, can be explained in two ways: On the one hand within a component, or-connections (e.g. SPB≥90% or DBP≥90%) are possible, and on the other, as a rule the percentiles were derived for normal-weight children (see: Measurement methods/exclusion criteria used in the IDEFICS study), for calculating the proportion that exceeds the 90th, respectively 95th percentile however, all children (including overweight and adipose children) were included.
 as well as the prevalence of metabolic syndrome (proportion of children who exceed th")
Additionally, a z-score standardization can be used to calculate a continuous score (IDEFICS MetS-Score) that combines the four components of metabolic syndrome. This additive score is defined as the sum of waist circumference sex- and age-specific z-scores (WC), HOMA-Index, the mean of the diastolic (DBP) and systolic (SBP) blood pressure z-scores, and the mean of triglycerides and HDL-C z-scores (the latter multiplied with -1, due to the inverse association between HDL-C and the metabolic risk profile):

References
- Cook S, Weitzman M, Auinger P, Nguyen M, Dietz WH. Prevalence of a metabolic syndrome phenotype in adolescents: findings from the third National Health and Nutrition Examination Survey, 1988-1994. Archives of Pediatrics & Adolescent Medicine. 2003;157(8):821-7.
- Viner RM, Segal TY, Lichtarowicz-Krynska E, Hindmarsh P. Prevalence of the insulin resistance syndrome in obesity. Archives of Disease in Childhood. 2005;90(1):10-4.
- Zimmet P, Alberti KG, Kaufman F, Tajima N, Silink M, Arslanian S, et al. The metabolic syndrome in children and adolescents - an IDF consensus report. Pediatric Diabetes. 2007;8(5):299-306.
- Ahrens W, Bammann K, Siani A, Buchecker K, De Henauw S, Iacoviello L, et al. The IDEFICS cohort: design, characteristics and participation in the baseline survey. International Journal of Obesity. 2011;35 Suppl 1:S3-15.
- Ahrens W, Moreno LA, Marild S, Molnar D, Siani A, De Henauw S, et al. Metabolic syndrome in young children: definitions and results of the IDEFICS study. International Journal of Obesity. 2014;38 Suppl 2:S4-14.
- Rigby RA, Stasinopoulos DM. Generalized additive models for location, scale and shape. Journal of the Royal Statistical Society: Series C (Applied Statistics). 2005;54(3):507-54.